Tag Archives: weight loss
OBESITY PREVENTION AND TREATMENT ON THE HIGH STREET
S. N. Kreitzman Ph.D, R.Nutr.
Howard Foundation Research
Treating overweight, but not-yet-obese people, in pharmacy, is obesity prevention on the high street. There are over 30 million overweight and obese people in the United Kingdom. Since no one ever became obese without first being overweight, it is important to provide real help to people at this stage. It is much less problematic to help people who do not have a massive amount of weight to lose and who also do not yet have some of the serious medical consequences associated with excess weight.
Pharmacy has become the prime location for weight management in the UK and Ireland. With the NHS ‘Call to Action’, pharmacy professional bodies are urging pharmacists to make their voices heard and shout about the good they do in improving people’s health. Take weight management for example. Helping people lose weight is not just about making them feel good but is also about preventing major long-term health problems, such as type 2 diabetes. This point was very well illustrated in a recent article in GP magazine that reported a staggering sevenfold rise in insulin use in type 2 diabetes over a nine year period.
But it seems that it’s not just the NHS that needs to hear what pharmacy has to say. The public do too. North London LPC was inundated with enquiries about a newsletter it had produced raising awareness of pharmacy services in the area.
So what does that mean to you as a pharmacist with a team already offering an established weight management service? Promote your service far and wide and show the public and the NHS what you’ve been doing to improve the health of the nation.
Fin McCaul, for example, is first and foremost a community pharmacist practicing in Manchester. He is also the Chairman of the Independent Pharmacy Federation and works for Bury CCG one day per week as its Long Term Conditions Lead.
Fin’s passion for independent pharmacy is second only to helping patients lose weight and stop smoking. With an average of 100 quits per year and well over 1000 patients helped through the weight loss service in his pharmacy, there is nobody better placed to talk about the opportunities and challenges for pharmacy now that Public Health commissioning has moved into the care of Local Authorities.
Delegation, motivation and marketing skills and advice for pharmacists and their team are just some of the benefits from his Stop Smoking/Weight loss clinics. At the 2013 Pharmacy show he organised a series of Patient Services Workshops delivered by Pharmacists who are successfully running weight services in their local community and want to share their knowledge and expertise.
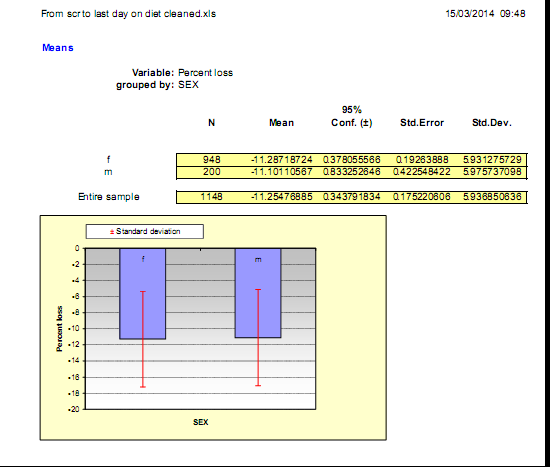
Fin’s expertise and results are not just anecdotes. He, along with many of the pharmacies treating overweight and obesity are generating extensive audit data from their weight management services. Results from one of his pharmacy audits below show the percentage of initial weight lost by over 1100 of his patients.
Pharmacy is an excellent provider of weight services for the community. Many overweight people in the BMI 25-30 range take advantage of pharmacy weight loss programmes recognising that they really work and confident that they are being monitored by healthcare professionals. Pharmacists’ expertise in weight management, however has proven extremely valuable for the treatment of obese and even the morbidly obese people. This is a group who could have qualified for bariatric surgery at great expense, risk and often compromised future life.
Effective weight loss absolutely needs to be monitored by knowledgeable healthcare professionals, because real weight loss is not benign. Type 2 diabetics, for example, who lose weight by compliance with a total food replacement diet programme, will induce remission of their diabetes within a few days and therefore continuing with hypoglycaemic medication can get them into serious difficulty. There are multitudes of patients taking medications such as warfarin or lithium, drugs which have a very narrow safety spectrum. Dieting can alter the absorption rate for these drugs so these patients need their dosages to be carefully monitored. There are some people who really should not be dieting at all. Pregnant women, patients with a recent history of surgery, stroke or heart attack are not logical candidates for weight loss. Effective weight loss should not be left to amateurs or internet sales. Healthcare professionals are needed, especially in pharmacy where continuous care can be provided even after the weight is lost, because weight maintenance requires the greatest attention and is not usually possible in a busy medical practice and appears to be almost impossible without professional help.
Although it is traditional to show successful dieters proudly occupying trousers which are now several sizes too large, there isn’t enough space to print over 13,000 examples. Results from this single audit of a group of pharmacies out of a collection of more than 2000 UK and Irish pharmacies currently treating overweight and obesity, is a vivid demonstration of the evidence base being accumulated for this absolutely essential community service from pharmacy.
Pharmacy is the only reliable community service providing and documenting long term weight management without the need major research grants or health service funding. Although there has been widespread press coverage for a £2.4 million grant by Diabetes UK to attempt to demonstrate that type 2 diabetes can be put into remission by effective weight loss, a fact that has been repeatedly reported in the medical press for over 30 years, pharmacies have been quietly and routinely succeeding with diabetes prevention and remission in their high street branches. Unlike bariatric surgeons, who need to justify the cost and risk of providing weight loss by surgical means on the basis of the phenomenal cost savings on the treatment of diabetes alone, weight loss in the pharmacy can accomplish the same results without massive expense and risk. And since total food replacement methods remove the substances of abuse for prolonged periods of time from those who may be suffering from a dopamine response to eating excess in their nucleus accombans , they don’t show the common addiction transfer syndrome that seems to be so common after bariatric surgery.
While activists continue to bellow about the size of soft drink containers, pharmacists are demonstrating how much their education and skills can be amplified by the convenience of access on the high streets of the UK. Pharmacy stands alone among the healthcare professionals in providing fantastic public health services such as smoking cessation, weight management, diabetes recognition, prevention and even treatment, medicines review, hypertension assessment and a host of other essential services very much needed in the real world. A major thank you is overdue.
PFD version: OBESITY-PREVENTION-AND-TREATMENT-ON-THE-HIGH-STREET
AUDIT RESULTS USING THE LIPOTRIM PATIENT TRACKER BY PHARMACIST GARETH EVANS
Audit Results using the Lipotrim Patient Tracker
by Gareth Evans
The current excitement generated by the press coverage of the Newcastle University study of diabetic patients using weight loss by a very low calorie diet to “cure” diabetes, necessitates a wider recognition of the well established programmes already available. The Lipotrim weight loss programme, monitored exclusively by healthcare professionals has been in extensive use in the UK for more than 25 years. A rapidly expanding network of nearly 2000 pharmacies currently offer the VLCD service and although many have used manual methods to audit their patients’ achievements, the newly provided Patient Tracker computer software for managing patient records has permitted continuous auditing of results and detailed evaluation of population subsets.
For example, in addition to auditing the total experience of patients enrolled in the pharmacist-run service, the results can be examined in many different ways. The cohort can be divided by gender, by age, by initial or final BMI, by amount or percentage of weight loss achieved, or by medical history (hypertension, diabetes, depression, thyroid problems etc.). The programme extends beyond weight loss, as there is a refeeding transition back to ordinary foods and a full maintenance programme, which is proving extremely successful in the pharmacy environment. With this Tracker audit tool, therefore, evidence is also available documenting the long term maintenance outcome after dieting.
As a pharmacist who has been using the Tracker to keep my Lipotrim patients’ records for some time now, I would like to share a current audit of my patients’.
Materials and Methods
Overweight or obese people requesting the programme are assessed for suitability on the basis of initial BMI and a detailed medical history. Those requiring medical cooperation, such as those with type 2 diabetes or medicated hypertension make suitable arrangements with their GP prior to dieting or are excluded. Those with contraindicated conditions, such as insulin dependant diabetes or pregnancy are excluded from the programme.
Suitable candidates follow a strict regime of total food replacement using nutrient complete formulas, essentially very low fat enteral feeds, with adequate fluid intake and only black tea or coffee permitted in addition. Appropriate prescribed medications are continued as well. No other foods, beverages or supplements are permitted.
Dieters are monitored and weights recorded weekly – only 1 week’s supply of formulas can be obtained at each visit and obvious non-compliance is corrected or the dieter is offered alternative weight loss advice.
Records are maintained on the Patient Tracker programme.
Results
Total Population of Dieters completing 3 or more weeks on Total Food Replacement
Mean Start Weight 91 kg – Mean End Weight 81 kg
Total weight lost to date of audit – 3865 kg
Table 1 N= 382 330 Females 52 Males
| Mean | Start wt | 91kg | Start BMI | 32.7 | End BMI | 29.0 | % wt loss | 10.8 |
| Median | Start wt | 88.2 kg | Start BMI | 32.0 | End BMI | 28.4 | % wt loss | 9.0 |
The next series of tables demonstrates the value of the Lipotrim service in overweight patients, reducing the likelihood of their progression to obesity, as well as obese, super obese, morbid obese or even super-morbid obese patients.
Table 2 N= 121 BMI 25-30
| Mean | Start BMI | 28.1 | End BMI | 25.4 | % wt loss | 9.3 |
| Median | Start BMI | 28.3 | End BMI | 25.4 | % wt loss | 8.0 |
Table 3 N= 141 BMI 30-35
| Mean | Start BMI | 32.4 | End BMI | 28.9 | % wt loss | 10.9 |
| Median | Start BMI | 32.3 | End BMI | 29.1 | % wt loss | 12.0 |
Table 4 N= 73 BMI 35-40
| Mean | Start BMI | 36.9 | End BMI | 32.4 | % wt loss | 12.9 |
| Median | Start BMI | 36.7 | End BMI | 32.6 | % wt loss | 11.0 |
Table 5 N= 29 BMI 40-45
| Mean | Start BMI | 42.2 | End BMI | 36.1 | % wt loss | 14.4 |
| Median | Start BMI | 42.0 | End BMI | 36.3 | % wt loss | 11.0 |
Table 6 N= 5 BMI 45-50
| Mean | Start BMI | 47.4 | End BMI | 37.2 | % wt loss | 21.2 |
| Median | Start BMI | 47.3 | End BMI | 36.9 | % wt loss | 22.0 |
Other subsets of the patient information that are of interest include:
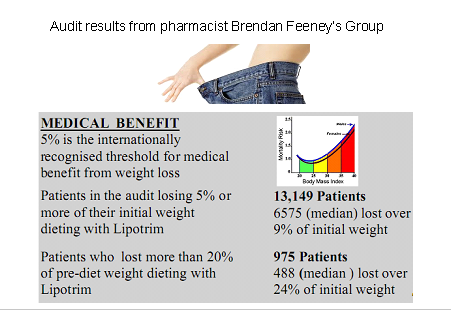
Table 7: Obese people who exceeded the 5% criterion for medical benefit of weight loss.
Tables 8and 8a: Some dieters choose to interrupt their diet for varied reasons and then return for a subsequent diet period. Their first and second dieting courses can be examined separately.
Table 9: After a period of weight loss, it is necessary to re-introduce carbohydrates in a controlled manner to minimise weight regain due to carbohydrate loading. Minimal weight change is expected despite reintroduction of normal foods. This phase is 1 week long.
Table 10: The Tracker software distinguishes between periods of dieting and maintenance providing evidence of minimal recidivism when patients are properly supported in the pharmacy environment.
Table 7 N= 231 BMI > 30 who lost 5% or more of initial weight
| Mean | Start BMI | 35.3 | End BMI | 30.8 | % wt loss | 12.7 |
| Median | Start BMI | 34.5 | End BMI | 30.1 | % wt loss | 11.0 |
Table 8 N= 78 Dieters who had 2 dieting courses First time
| Mean | Start BMI | 32.1 | End BMI | 29.1 | % wt loss | 9.0 |
| Median | Start BMI | 31.2 | End BMI | 28 | % wt loss | 7.5 |
Table 8a N= 78 Dieters who had 2 dieting courses Second time
| Mean | Start BMI | 31.1 | End BMI | 29.6 | % wt loss | 4.7 |
| Median | Start BMI | 29.7 | End BMI | 28.1 | % wt loss | 3.5 |
Table 9 N= 140 Refeeding week
| Mean | Start BMI | 27.5 | End BMI | 27.4 | % wt loss | -.2 |
| Median | Start BMI | 26.6 | End BMI | 26.6 | % wt loss | 0 |
Table 10 N= 249 Maintenance after dieting
| Mean | Start BMI | 28.1 | End BMI | 28.1 | % wt loss | 0.1 |
| Median | Start BMI | 27.2 | End BMI | 27.0 | % wt loss | 0 |
Patients who are medicated for various weight related ailments can often be considered as different categories of patient. Many hypothyroid patients have experienced great difficulty with weight management. Depression and hypertension often have a weight component in the aetiology of the problem.
Table 11: Examines patients on medication for hypertension
Table 12: Examines patients on medication for hypothroidism
Table 13: Examines patients on medication for Depression
Table 11 N= 22 Patients with High Blood Pressure
| Mean | Start BMI | 36.2 | End BMI | 32.0 | % wt loss | 11.6 |
| Median | Start BMI | 37 | End BMI | 32.2 | % wt loss | 8.5 |
Table 12 N= 9 Patients with thyroid hormone replacement
| Mean | Start BMI | 34.5 | End BMI | 29.4 | % wt loss | 14.2 |
| Median | Start BMI | 34.7 | End BMI | 28.9 | % wt loss | 10.0 |
Table 13 N= 13 Patients with Depression
| Mean | Start BMI | 33.2 | End BMI | 28.2 | % wt loss | 13.0 |
| Median | Start BMI | 32.2 | End BMI | 28.9 | % wt loss | 11.0 |
Discussion
The extreme flexibility of the Patient Tracker software, in addition to documenting and visualising each individual patient’s experience, allows for presentation of evidence of the weight loss achievements of cohorts of patients. This has become important for commissioning and the new ability of grouping patients from an individual surgery permits certification to the surgery of the collective progress of their patients, These results can be of value for CPD as well.
As can be seen from the multiple tables presented as illustration, the percentage of initial weight lost generally averages well over 5% and in most cases over 10%. Even the median values, which documents the half-way values of the ranges, are generally very close to the mean. Successful weight loss is found even in the extremely high BMI patients, who are usually refractory to weight management attempts.
In addition to demonstrating the successful loss of weight by the dieters, regardless of the sub-category for grouping, it is important to note that even though there are some variations in patients’ experiences with re-feeding (Table 9) and follow on maintenance (Table 10), the overall lack of weight regain from the patients post-diet demonstrates the value of the pharmacist and the Lipotrim programme for long term weight control.
Conclusion
Despite the fact that these results reflect the efforts of a single pharmacist in a programme that currently lists nearly 2000 pharmacies throughout the UK and Ireland, it is important to have the tools that can satisfy the need for documentation of achievement in this era of evidence-based treatments. The success of this pharmacy service has considerably enhanced my professional satisfaction as a pharmacist.
TREATING DIABETES: RAPID CONTROL WITH WEIGHT LOSS
There is now a pandemic of obesity, and the problem is causing increasing levels of type 2 diabetes. Cooperation with effective pharmacy weight loss programmes can reliably provide rapid and potentially long-term clinical benefits from weight loss. Stephen Kreitzman and Valerie Beeson explain how Lipotrim can help
diabetes is a progressively debilitating disease, often requiring increasingly aggressive therapy. The treatment protocols with oral hypoglycaemics usually lead to increasing body weight. The increased weight degrades insulin sensitivity and can ultimately lead to a need for insulin. With insulin, a common outcome is yet further weight gain, and the disease gets increasingly worse. This entire cascade of events can be avoided.
There are really two basic facts to consider. The first is that type 2 diabetes is a disease that has a primary aetiology, which is close to 100% reversibility related to excess body weight. The second fact is that diabetic patients can lose enough weight within a few days to bring their blood sugars under control and enough further weight within weeks to crucially reduce cardiovascular risk factors and apparently keep the disease in remission, even with some weight regain.
Achieving a maximum safe rate of weight loss
Modest reductions in calories can theoretically result in weight loss. Of course, the modest reduction has to be from the equilibrium level, not from current intake. If a person is overeating by 2,000 calories a day (very common in the obese), a modest reduction in calorie intake will not cause weight loss.
There is a maximum rate of weight loss for any individual. A total fast provides zero calories and therefore requires that all the calories necessary for life come from the body fuel reserves. A total fast, however, provides no nutrients, and since an obese patient has a far greater reserve of calories than stores of other essential nutrients, a total fast is out of the question as a treatment. To be healthy, a diet has to supply adequate essential amino acids, essential fatty acids, vitamins, minerals and trace elements. A total fast cannot be a valid treatment for obesity. The simple idea of reducing fat levels in an enteral formula solves both the calorie and the nutrient problem. An ideal nutritional product with the absolute minimum of calories consistent with a healthy diet is achieved. Lipotrim is an example of such a product, providing a maximum safe rate of weight loss. The literature on safety and efficacy is massive. The time has really come to pay attention to it.
There is also extensive literature on the beneficial effects of weight loss on cardiovascular risk factors, on blood lipid profiles and on blood pressure. Managing weight in practice, however, can be time consuming. The beneficial results from substantial and rapid weight loss on the glycaemic control and the cardiovascular risk factors more than justify consideration of this approach. Cooperative efforts with local pharmacists, however, benefit patients, pharmacists and also the primary care
providers.
Weight is extremely important to patients and has a critical influence on the clinical course of type 2 diabetes. It would appear prudent and considerate to give diabetic patients an opportunity to lose weight using Lipotrim under your own care or encourage them to seek care from a local pharmacist.
Stephen Kreitzman PhD RNutr, Valerie Beeson Clinical Programme Director
PDF version: 4-TREATING-DIABETES-RAPID-CONTROL-WITH-WEIGHT-LOSS.pdf
SUCCESSFUL WEIGHT MANAGEMENT IN PRIMARY CARE
Stephen Kreitzman Ph.D, (UK Registered Nutritionist) & Valerie Beeson
Howard Foundation Research Ltd. Cambridge
Weight loss goals are not utopian dreams. Diabetics off their drugs in days. Blood pressure reduced.
Patients qualifying for elective surgery. Depression tempered. Fertility enhanced. Patients capable of a more active lifestyle.
Blood lipid profiles improved. Self esteem and quality of life enhanced. These are goals achieved routinely by weight loss.
They are being achieved by your GP colleagues and by your pharmacist colleagues. And it isn’t necessary to wait for PCT funding.
Obesity management is basic science. People have to eat a lot fewer calories than they use. That is, they have to maintain a large calorie gap. Calories do count and the laws of physics can not be violated regardless of the macronutrient profile of the foods eaten.
EXERCISE
Obesity management also requires more than exercise at the levels realistically achievable by seriously overweight people. Obesity management requires an understanding of the full impact of extra ener-gy expenditure – even in the unlikely event that the extra expenditure is substantial – when energy intake continues to be excessive. Obese people have eaten and in all probability are still eating more calories than they need.
Their excess intake can often be measured in the many hundreds of calories. It takes a very large amount of exercise to cope with these excess food calories before any contribution can be made from the body’s fat stores and cause weight loss. After coping with the excess food calories, it takes an additional deficit of 3500 calories to consume a single pound of body fat. Often it takes a major effort for obese people simply to accomplish activities that other people take for granted. To expect obese people to dissipate very large numbers of excessive calories by exercise is naïve. To risk the heat overload generated by intensive exercise in people whose fat mass, a considerable and effective insulation material, dangerously impedes heat loss, is unwise.
WEIGHT MANAGEMENT IS ACHIEVABLE
Weight loss of significant magnitude, even in seriously obese patients, is achievable either in your own practice or with the assistance of a rapidly growing number of trained pharmacists. Pharmacists over the last 3 years are getting excellent
results running the same professional Lipotrim prot-ocols as have been run exclusively in UK general practices and hospital clinics since 1987. The parliamentary all party pharmacy group (APPG) has called for greater pharmacy
involvement in obesity management and pharmacists are responding to that call.
PHYSIOLOGY
There are some fundamental concepts of physiology that must be understood in order to treat weight problems successfully. The most frequently misunderstood concept, even by professionals, is the rela-tionship between weight loss and body fat loss. They are not the same. Weight loss can be achieved with a diuretic, by sweating and even by exercise, without any loss of body fat. The primary fuel providing energy for the body is glucose and it’s reserve polysaccharide, glycogen. These carbohydrates are stored in the body in the liver, muscles and fat cells. Fat people can store a considerable amount of glycogen in their numerous fat cells, in comparison with thin people who usually only store about a pound or two of this carbohydrate fuel. It is extremely important to recognize that the carbohydrate fuel is stored in a highly hydrated state – 3-5 parts water to each part of glycogen. This results in what amounts to a diuresis as glycogen is utilized. Instead of 3500 calories required per pound of fat weight lost, weight lost as glycogen and its associated water requires only about 360 Calories per pound, 10% of the energy deficit. Further, repletion of glycogen and water weight is rapid and necessary. Shifting glycogen and water weight on and off should not be confused with obesity management.
WEIGHT LOSS USING NUTRITIONAL REPLACEMENT THERAPY
Obesity management requires enough of a calorie deficit to deal with 7700 kcal per kg of fat weight lost. An individual of
average height has to lose about 3 kg of weight to reduce BMI by a single unit. Therefore a calorie deficit of energy use
compared with intake has to reach about 23,100 kcal in order to achieve one unit reduction in BMI. This can most
realistically be achieved by maximizing the calorie gap between intake and expenditure. The absolute maximum is obviously achieved by a total fast, however, a total fast provides no essential nutrients and would therefore lead to serious health problems and ultimately death. Energy intake is not required since each stone of excess weight is a store of over 37,000 kcal. Providing the essential nutrients of vitamins, minerals, trace elements, essential amino acids and fatty acids entails providing some calories, therefore the maximum safe caloric gap is defined by the calorie content of an intake providing all essential nutrients in adequate amounts. This is achieved, by a carefully designed formulation, in approximately 400 kcal per day. Nutritional replacement therapy formulations have a long history of safe and effective maintenance of patients for prolonged periods, however, they are ordinarily designed to provide enough energy for weight maintenance or even weight gain. Drastic elimination of fat calories from these formulations, however, can provide for essential nutrition while supporting sustained weight loss. This is the basis for the success of the Lipotrim obesity management system.
OVERCOMING “ADDICTIVE” EATING BEHAVIOUR TO ACHIEVE LIFESTYLE CHANGE
It is becoming increasingly apparent that excessive consumption of food shares many of the characteristics of addictive behaviours towards other substances of abuse.
Whether it be tobacco, alcohol or drugs, once excessive consumption is evident, the only way to have any reasonable chance of regaining control is to stop completely the substance being abused. While total abstinence is achievable and
generally recommended when dealing with these other substances, obese patients are usually encouraged to control their excesses by consciously overriding their drives to eat in the face of the temptations of continued exposure to food. The frequent failure to achieve this over a prolonged period is not surprising. What is required is a complete withdrawal from the lure of food for as long as possible. This is achievable using a nutritional replace-ment formulation, which is not generally perceived as food. When food avoidance is complete, it has the dramatic effect of re-establishing more cont-rolled behaviour towards food when traditional food is reintroduced. This positive benefit is commonly seen, for example, when people substitute skimmed milk for whole milk in tea or coffee. It is rare for these people to reintroduce whole milk again. Long term lifestyle change in eating behaviour becomes considerably more likely when there is a complete break from the substance of abuse. Patients adhering strictly to the Lipotrim total food replacement formulations have a vastly improved record of post diet weight control compared with historic approaches.
ADVANTAGES OF PHARMACY OVER IN-HOUSE TREATMENT
While many prac-tices prefer to manage their own obese patients with Lipotrim, there are practical limitations that often
make it desirable to utilize a pharmacy. In addition to the obvious considerations of time availability, where a pharmacist could treat a patient at almost any time during long opening hours, time available in the surgery is generally much more constrained. As a result, treatment is often restricted to the most severe cases where the weight has contributed to some co-morbid condition such as diabetes or when the patient faces a long delay in attaining surgical help unless weight is lost. With almost a quarter of the adult population now clinically obese and over half of the population overweight, the treatment burden can rapidly become overwhelming for the practice. Also, it is widely recognized that prevention by intervention before the patient becomes obese is preferable. Weight is not considered a medical problem below BMI30 and it is hard to justify practice time for lower weight patients who are otherwise still heal-thy. Similarly, once a patient has achieved weight loss and is at a normal weight, they are greatly in need of further, long term maintenance assistance, but this is difficult to justify in practice since they are now at a normal weight. There are, however, some medical conditions where either total management in practice or a shared management with the pharmacist is necessary. This is most dramatic with type II diabetes treated with oral agents. There is a p r e c i p i t o u s normalization of blood sugar, usually within the first 3-5 days of Lipotrim treatment. Continued use of the oral agents in the presence of normal sugars can become problematic and therefore medication needs to be stopped or severely reduced. This cannot be done by the pharmacist without the cooperation of the primary care doctor.
THE FACTS ARE IN THE LITERATURE
Obesity has finally become recognized as a major public health problem and the primary care team is being looked upon
to deal with it. The approach to obesity treatment briefly outlined in this short piece is extremely well documented in what has become a vast scientific and medical literature. Weight losses of about 1 stone per month for women and even
more for men are not only achievable, but are also expected. They are proven safe when used under knowledgeable
care and there is no longer any excuse for patients to endure futile attempts to manage their obesity. Considerable
discussion of the medical science can be found on the UK Food Education Society web site at www.foodedsoc.org.
PDF version: 2-5-successful