Pat Miles, David Kerr
Introduction
The therapy of obese patients with poorly controlled diabetes is a complex area. Despite the best efforts of healthcare professionals and patients, therapy is too often associated with repeated failure, which can give rise to frustration and sometimes despondency. Very low calorie diets (VLCDs) have been advocated for this population group. This article looks at the process and outcomes of one VLCD programme. The results support the wider adoption of VLCDs, but there are significant resource implications which are also discussed.
The treatment of the obese individual with poorly controlled diabetes is a common and perplexing problem. Wading in with ever increasing amounts of insulin without giving thought to ameliorating the inevitable weight gain will cause desperation in the multidisciplinary team and despondency in the patient. Very lowcalorie diets (VLCDs), of <800 kcal perday, are designed to achieve substantial weight loss while preserving lean body mass and are typically associated with a 20 kg weight reduction in three months (NTFPTO, 1993). Unfortunately, regain of half to two-thirds of the initial weight loss is common within 12 months after cessation of the diet, although there may be longer term benefits in terms of a reduction in the need for medication in obese individuals with diabetes (Wing et al, 1994). Recently, Paisey et al (1998) compared VLCD with a traditional intensive dietary regimen in 30 obese (BMI>30) patients with diabetes and 19 obese controls without diabetes. After four months of VLCD, subjects were switched to a low-fat diet and continued to be seen weekly by the multidisciplinary team. Weight loss was substantial and maintained after cessation of VLCD (mean 14kg at 12 months), and 14 of the 15 patients who had chosen VLCD had normal blood glucose and fructosamine levels despite stopping all medication. For four patients with recent-onset diabetes, normalisation of blood glucose levels was sustained for 12 months.
Study aim
A pilot study was carried out to examine the effect of a VLCD programme on a group of obese (BMI30) patients with diabetes. These patients remained obese despite enormous efforts by the multidisciplinary team (including primary care). Usually, there was also poor glycaemic control. Method Between January and June 1999, 24 patients aged 29–76 years were enrolled into Lipotrim (Howard Foundation Research, Cambridge, England), a VLCD programme which gives 450 kcal per day for women and 600 kcal per day for men. For entry to the programme, each patient had to:
- Understand the programme
- Desire to take partUndertake to attend weekly individual and group sessions
- Have family support
- Be desperate or determined to lose weight.
The product was available from the hospital at a cost of £18 per week for women and £24 per week for men. The expenditure for each patient was offset against money saved by not purchasing normal food. Lipid-lowering medication was stopped on entry to the programme. Weight, blood pressure and urinary ketones were measured once weekly up to refeeding then weight and blood pressure were measured at every patient contact thereafter. Lipid levels and HbA1c were measured at the start of the programme, every month for the first six
months then at three-monthly intervals for the next six months. Patients were expected to attend the individual and group sessions at each visit (every week). In the individual sessions with the nurse, patients could discuss any problems they had encountered (Figure 1). Group sessions provided support, an opportunity to exchange experiences and preparation
for refeeding. The dietitian was involved around the time of refeeding, to reinforce product literature from the company. Most patients refed at 3–4 months, and then followed a low fat healthy eating plan. After refeeding, follow up continued weekly for the first month, then every 2–4 weeks (frequency at the patient’s discretion). However, group sessions stopped at six months into the programme.
Results
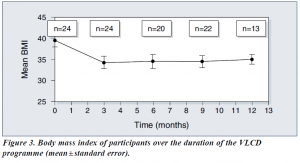
Average body mass index (BMI) was 39.5 at the start of the study.
Of the 24 patients:
- 16 were being treated with insulin
- 14 were hypertensive and were receiving appropriate medication
- 14 had dyslipidaemia and were receiving appropriate medication
- 2 were suffering from sleep apnoea requiring continuous positive airways pressure
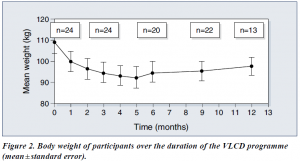
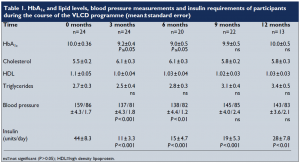
Following the introduction of VLCD, there were significant reductions in body weight (Figure 2) and BMI (Figure 3). Data on HbA1c levels, plasma lipids, blood pressure and insulin requirements of programme participants are shown in Table 1. Plasma lipid levels remained largely unchanged. Only four patients restarted lipid-lowering medication after refeeding.
Blood pressures dropped significantly within the first week, and adjustment of antihypertensive medication was necessary on a regular basis. Eleven patients stopped all antihypertensive medication. For most patients, ketone levels were moderate to high during the VLCD (indicating adherence to the programme and utilisation of fat stores). Insulin doses were decreased by two thirds on commencement of the programme, and this seemed to work well, with insulin doses continuing to decrease as weight loss proceeded. Most patients who remained on insulin were changed to nocte insulin
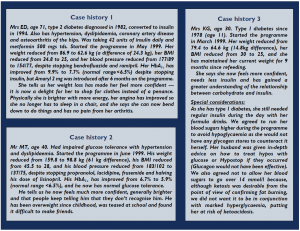
when their requirements were less than 14 units a day. Sulphonylureas were also halved or stopped on commencement of the programme. Only 13 patients completed follow up for the 12 months of the programme. The three case histories (see page 111) provide further detail about some of the patients in the programme.
Discussion
Benefits of VLCD
VLCDs can be an effective method of reducing weight, improving glycaemic control
— at least in the short term — and reducing the need for concomitant medication in
obese people with diabetes. They can also allow individuals to gain insights into the potential benefit of weight reduction and to learn about the relationship between food and obesity. When asked why this diet had worked while all others had failed, our patients said that it was easier to have no food at all, than to try to make choices from food offered, particularly on social occasions. Also the rapid weight loss experienced on the programme was positive reinforcement, together with the feeling of ‘wellbeing’ experienced as a consequence of ketosis (Burley et al, 1992).
Some considerations
It is well known, however, that helping someone to maintain weight loss is often the most difficult and disappointing task (Wing, 1995). In addition, the process is very time consuming for any healthcare professional involved. This pilot project to examine the effectiveness of VLCDs involved seeing 24 patients every week for 3–4 months, then at least monthly for the following nine months. We have only touched the ‘tip of the iceberg’ in our clinic population. If this service were offered to all of our obese patients (at least 60% of the total), a 50% uptake would involve 2250 patients who would require 11 whole time equivalent healthcare professionals just to provide weekly visits! In practice, this would be unrealistic and unlikely to attract funding, though one could argue that treating the root cause of the problem is far better than attempting to treat the effects. Putting VLCD into practice In many areas, primary care is offering Lipotrim to its obese patients. If the expertise of practice nurses and community dietitians in using this product could be built up, and the diabetes team was available for advice on medication changes for people with
diabetes, then it could be possible to offer this service more widely and cost effectively.
However, because of the additional risks of hypoglycaemia and ketoacidosis in patients with type 1 diabetes, we feel that they should only be offered the programme under the supervision of an experienced diabetes team, and then only if the patient is able to self-adjust insulin appropriately and understands the risks.
Conclusion
This study advocates the use of VLCDs for reducing weight and improving glycaemic control in obese people with type 2 diabetes (as well as carefully selected people with type 1 diabetes under close supervision). VLCDs can also reduce the need for concomitant medication. While on a VLCD, individuals can become empowered through their increased awareness and knowledge of their diabetes and the positive feedback provided by the rapid weight loss. It is likely that lack of time would limit the widespread adoption of the VLCD service used in this pilot study. However, the potential benefits of VLCD make it worthwhile to try to produce a costeffective service, perhaps by increased primary care involvement.
PDF Version: bournmouth-miles-kerr